
Bunions, also known as hallux valgus or hallux abductovalgus (HAV) are a common foot problem. Visibly, there is a lump on the side of the foot below the big toe. This is what is affectionately known as the “bunion”. But a bunion is just one part of a bigger angular “deformity” of the first metatarsal, the big toe and their joint called the first metatarsophalangeal joint (1st MPJ for short, or big toe knuckle). Bunions make your foot wider. Some bunions are painful, many are not. In fact, the degree of the deformity is not always correlated to the degree of pain. Unsurprisingly, bunions and blisters often go together, particularly in certain shoes and with increased activity. Perhaps surprisingly, it’s often not the bunion itself that gets the blisters – at least not where you would expect it. So, let’s unpack this bunion issue and talk blisters.
What Does A Bunion Look Like?
Bunions are a slowly progressive deformity. You don’t get one in weeks or months, and you certainly don’t wake up one day with a bunion. Bunions and the HAV deformity develop over many years.
Contrary to popular belief, they aren’t just a lump of bone that grows out the side of the foot. Hallux abductovalgus starts with a deviation of a bone in the midfoot – at the base of the first metatarsal (at the first metatarsocuneiform joint). Due to an instability of some sort at this joint, the first metatarsal begins to slowly angle outwards – towards the other foot. As it angles outwards, the end of the bone, the metatarsal head, becomes prominent. It’s not extra bone – it’s just normal bone that now sticks out more than it used to.
But it doesn’t finish there. You’ll notice the big toe bends towards the second toe. And if you’re really observant, you’ll notice the big toe rotates a little too. (1) The big toe is pushed towards the second toe by your shoe and ground reaction forces. As the big toe moves towards the second toe, this further exposes the head of the first metatarsal. Again, the bony protuberance of the bunion is not extra bone, it’s just normal bone that now sticks out more.


Tailor's Bunion (Bunionette)
While bunions mostly affect the big toe knuckle, bunionettes (tailors bunions) are a similar deformity on the other side of the foot - at the little toe knuckle, or 5th MPJ.

Tailors bunion on both feet. Notice how the bunion bulges over the insole. It's no surprise that perfectly-fitting shoes are difficult to find.
Diagnosing A Bunion Generally, the diagnosis of bunions can be made visually. Still, podiatrists will sometimes order a simple weightbearing x-ray to get more information about the nature of the problem. From this, they can measure the degree of the angulation and confirm the degree of arthritic joint degeneration, if any.
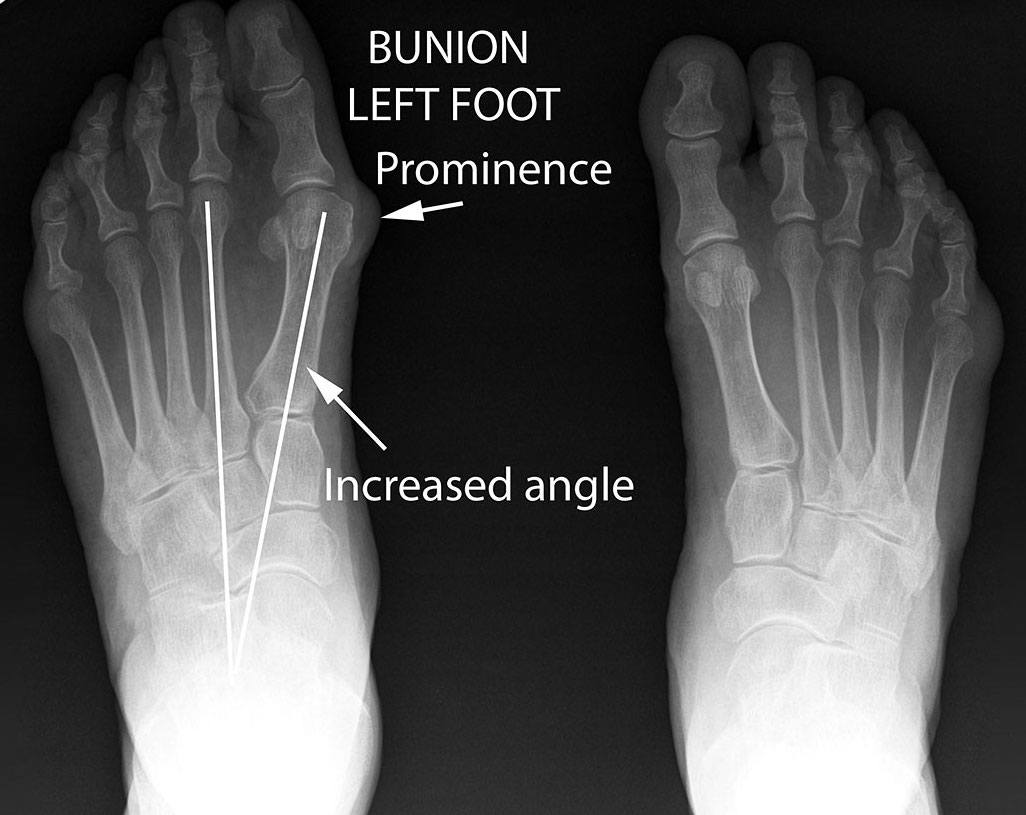
Bunion left foot / no bunion right foot: The intermetatarsal angle measures the outward deviation of the first metatarsal. Remember, the angular deformity of hallux abductovalgus (bunions) starts at the base of the first metatarsal - at the metatarsocuneiform joint. The bunion prominence is evident at the head of the first metatarsal p>
So What Causes Bunions? Contrary to popular belief, it’s not just about tight shoes. There is no single specific cause of bunions – they are multifactorial. Actually, for such a common foot problem, you may be surprised at how much is NOT known about the cause of bunions. But the general consensus, highlighted by a recent episode of PodChat Live with two experienced bunion surgeons, is twofold:
Firstly, genetics. Bunions often “run in the family”. It is known to be autosomal dominant with partial penetration. Research suggests up to 90% of people with bunions confirm a family history (2) (3). While you’re not born with bunions, there seems to be some structural or mechanical reason that you inherit for there being a high chance of bunions developing.
And secondly, there is an instability at the base of the first metatarsal (at the first metatarsocuneiform joint) (4). There’s something about how the foot behaves at this joint – something about either this joint’s mobility or the shape/angle of the medial cuneiform that predisposes to HAV and bunion development.
While a combination of genetic and external factors can be responsible, here are some of the contributing stressors and potential risk factors include:
- Ligamentous laxity – Joints rely on ligaments for structural stability. When ligaments are loose, it’s easy to see how weightbearing joints, like those in the feet, lose some structural support.
- Flat feet – I’m talking in very simplistic terms here when I say “flat feet” can cause bunions. Certainly, not everyone with flat feet get bunions. In fact, lots of people with high arches get bunions. It’s beyond the scope of this article to go into full detail. But there are some structural and mechanical reasons for bunions to develop more readily when the foot functions in certain ways.
- Shoes that are too small or too tight – This is the commonly-held cause of bunions. This includes hand-me-down shoes from older siblings to high heels and shoes with pointed toes. This certainly doesn’t help as these shoes tend to push the big toe over towards the other toes. But not everyone that has bunions has worn tight shoes. And plenty of people who wear tight high heeled shoes don’t get bunions.
- Long periods of standing and weightbearing activities – If you have any structural or mechanical reason to get bunions, it makes sense that the more you’re on your feet, the faster it will develop.
- Arthritis – While arthritis can be a consequence of long term HAV deformity, diseases such as rheumatoid arthritis can destabilise joints and accelerate joint degeneration.
- Injuries to the foot – This is the main reason people get a bunion on one foot and not the other. My father had a bunion and hammertoe on his right foot after it was run over by a car in younger days.
- Congenital anomalies – For example, metatarsus adductus.


Why Do Bunions Hurt?
Perhaps surprisingly, bunions often don't hurt. But when they do, pain can occur in one of three places:1) Skin
The skin over the lump of the bunion can redden, rub, blister, callous or less commonly, develop corns. The tighter the shoe, the more it will press and rub on this widest part of your foot. However, just as common, if not more common, are callouses and blisters under the lower edge of the bony prominence. This is where the lump protrudes over the side of the shoe’s sole. The skin under the edge of the protuberance is subject to localised higher weightbearing pressure.
Edge callous, blisters and rubbing with bunions
2) Subcutaneous Soft Tissue (Bursitis)
This is very common over the bunion lump when tight shoes are worn. With the concentration of shoe contact pressure, the bursa overlying the lump fills with fluid as a kind of protective response, and inflames. If you ever notice your bunion appears bigger and redder from time to time, this is bursitis. Bunions without bursitis feel hard and bony. With bursitis, the feeling when you press on them is soft and spongey, and quite tender. Wearing shoes that are appropriately wide is the key to minimising bursitis pain.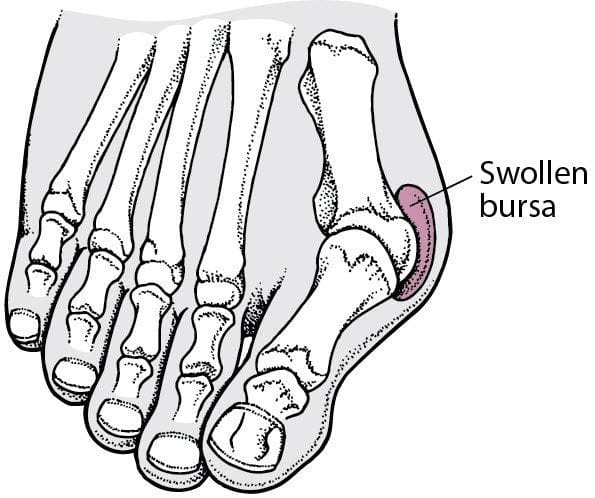
Bursitis overlying bunion
3) Joint
A deeper joint soreness can also occur with bunions, without the more surface symptoms. This is related to the function of the joint itself rather than shoe fit and outside pressure on the bunion. Over time, progressive degenerative joint changes can lead to a progressively stiffer joint and a more painful joint. But not always. Orthotics and other mechanical interventions can often help maximise function at this joint and relieve pain.
Severe bunion deformity. Notice the deviation of the big toe which exacerbates the prominence of the metatarsal head (the bunion).
Where Can You Get Blisters On Bunions (And Why)?
Okay, let’s focus on the skin now, and the blisters you can get associated with bunions.Blisters on the Bunion Itself
A bunion makes the forefoot wider. As mentioned earlier, blisters aren’t as common on the actual bony protuberance where the foot is its widest. Blisters are much more common under the bony protuberance, where the bunion bulges over the sole of the shoe. We call these edge blisters.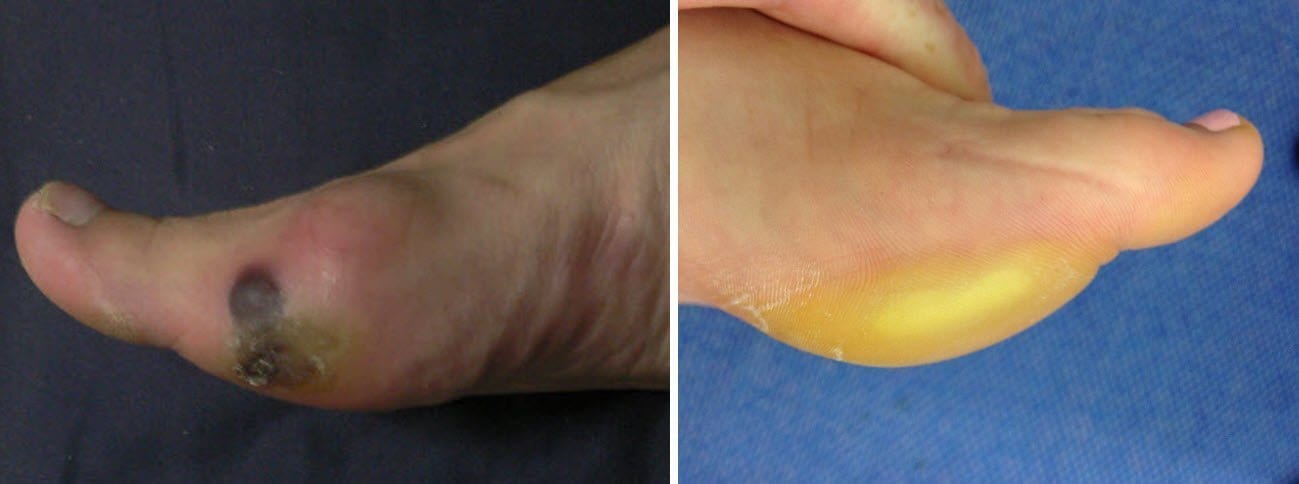
Bunions and blisters: Edge blisters under the edge of the blister
The Way to Prevent Edge Blisters is Two-Fold.
Firstly, you have to reduce pressure as much as you can. This means, do everything you can to get shoes wide enough to fully accommodate your bunion. So that it doesn’t bulge over the sole of the shoe. That easier said than done. Orthopedic shoe stores will provide extra width shoes. And orthopedic shoes can look much less dowdy and medical these days. When it comes to athletic shoes, ladies can buy men’s shoes – they’re wider for the same length. However, excellent shoe fit can be impossible – even with a moderate bunion. It can legitimately be impossible to negate the bulging of the joint over the sole. This means there will always be a concentration of pressure. But it doesn’t mean you need to console yourself to a lifetime of blisters. Even if you’re very active. Next, take care of friction levels (below).
This isn't a bad bunion or blister. But the bunion joint is too wide for the insole, and that means too wide for the shoe. This will be even more noticeable when standing. The bunion will actually bulge over the edge of the she's sole, creating a concentration of pressure. The more you're on your feet, the more likely the skin under the edge of the bunion will callous and/or blister. p> p> Secondly, you need to reduce friction levels as much as you can. I recommend ENGO Blister Patches using the Two-Patch technique. One patch goes on the horizontal insole, the other on the vertical shoe upper surface. That way, you created a long-lasting smooth interface right where it’s needed. Alternatively, Armaskin socks could achieve a similar result. If you choose to use powders or lubricants, be sure to reapply them every hour or so.
In addition, there are other slightly less effective preventing techniques. You could tape the bunion joint with a thick rigid tape. It’s a tricky joint to tape, even with a flexible tape, but thick and stiff tapes like a thick stiff moleskin will help most. Taping may help a little, but not as much as the pressure and friction management strategies already mentioned. Similarly, donut pads tend to be not as effective for bunion edge blisters as other blister locations. One thing I would recommend though is keeping any edge callous down to a minimum. This alone won’t stop a blister from forming but it will be much less painful than if you have a big chunky callous over your blister. Apologies for the quality of the video, but this is a good taping technique for bunion blister prevention, demonstrated by Anna Beetham.
Other Places You Can Get Blisters Because of Bunions
Not only does the forefoot get wider because of the bunion lump, the big toe also deviates towards the other toes. As it does, there becomes less and less room for the other toes. The result is one of three things. I’ve linked each blister location to the page discussing prevention of that blister – so go ahead and click the links for further information. Okay, one of three compensations can happen when the big toe starts to encroach upon the other toes. Either:- The second toe buckles upwards into a hammertoe. This happens to make room for the big toe to move into. This is the most common compensation. Corns and blisters can occur on:
- Under the big toe: Particularly on the medial edge due to the deviation of the big toe.
- The top of the second toe: because it sticks up more.
- The tip of the second toe: because it has now become weightbearing.
- Under the toenail of the second toe: now the tip of the toe is weightbearing, the nail gets pushed back with each step.
- Under the 2nd MPJ: as a toe buckles up, the MPJ becomes more prominent under the foot.
- All the lesser toes skew laterally towards the little toe. With the little toe constrained by the shoe, interdigital pressure increases and toes can tuck under the adjacent toe. The most common blisters are:
- On the outside of the little toe: as it abuts the shoe.
- Interdigital blisters: due to the increased pressure between the toes.
- Pinch blisters: one toe curls under the adjacent toe and the soft tissue is compressed.
- The big toe lifts up and sits over the second toe. This is much less common. But when it does, the most common blisters are:
- Between the first and second toe: because the shoe presses down on the big toe and pushes it harder onto the underlying second toe.
- Under the big toenail: Obviously the toenail is pushing into the top of the toebox.

Bunion Treatment
Blisters aside, what can be done about the hallux abductovalgus deformity itself? Many forms of treatment exist for bunions and range from non-invasive to the surgical. Some of these include:- Appropriate Footwear Choices. If current shoes are an issue, finding roomier and more accommodating footwear can significantly reduce pain and potentially even the progression of the deformity. Width of the forefoot is what you’re looking for.
- Cushions and Padding. A variety of options exist, such as foam or gel covers for the bony protuberance. It won’t fix the bunion but may alleviate superficial symptoms.
- Interdigital Wedges. A wedge between the first and second toes will help hold the big toe straighter. The bulkier the wedge is, the straighter it will hold the big toe. But it won’t stop or correct the HAV deformity. Gosh, if only it was that easy! Also, while a wedge provides a beneficial force on the big toe, it necessarily provides a force to the second toe -pushing it towards the other toes. This can become problematic.
- Splints. Bunion splints aim to hold the big toe straighter and stop it from deviating towards the other toes. Unlike wedges that push the second toe, they attach further up your foot in order to push the big toe out, leaving the second toe alone. While they won’t stop the bunion from developing further, and while they certainly don’t correct it, some people find they do provide some relief of symptoms.
- Orthotics. Inserts and orthotics can be used to address biomechanical reasons for bunion development – the instability of the first metatarsocuneiform joint. Both over the counter and custom-made formats can be used. It is highly recommended that you see a podiatrist – an expert in foot anatomy and function – to determine if orthotics are appropriate in your circumstance. And if so, to choose the specific design elements your feet require for them to work adequately.
- Surgery. Of course, sometimes conservative treatments don’t do the trick. And you’re looking for a permanent resolution to your bunion. Being a bony deformity, only bony surgery can truly “correct” a bunion. There are basically 3 reasons people opt for surgery. Either:
- The bunion is painful and conservative options fail or are inappropriate.
- The compromise in footwear is not possible or is inadequate.
- The deformity is a significant psychological burden.
- Bone takes 6-8 weeks to heal.
- You are never completely off your feet. In fact, you’ll be able to walk from day one, albeit minimally. Your surgeon will very likely give you a special shoe to walk in, and a special way to walk, so as to preserve the surgical site. You’ll gradually increase the amount you can walk as the weeks go by.
- The first two weeks are critical – you don’t want to injure the foot or do too much as the surgical site is still quite fragile.
- Generally, you get one bunion done at a time (so you have a good foot to lean on)
- Well after the pain or discomfort of the surgery passes and you’re able to walk and do all the things you used to, swelling may linger and limit you from getting into tight or non-adjustable shoes, just for a little longer than you might expect.
Wrapping Up
Wow, there’s a lot of bunion info here. While it’s my aim to explain all about blisters, this is such a common affliction and one where people have a lot of questions. Has it answered all your questions – all your bunions and blisters questions? If not, pop them question in the comments section and I’ll do my best to answer them. p> p>References
- Clinical Evaluation of Hallux Abducto Valgus: www-s3-live.kent.edu/s3fs-root/s3fs-public/HV-ch-05-Clinical-Evaluation-of-Hallux-Abducto-Valgus.pdf
- 3. Pique-Vidal C, Sole MT, Antich J. Hallux valgus inheritance: pedigree research in 350 patients with bunion deformity. J Foot Ankle Surg. 2007; 46(3):149-54.
- Lee CH, Lee S, Kang H, Jung DE, Song YM, Lee K, Lee K, Hwang J, Sung J. Genetic Influences on Hallux Valgus in Koreans: The Healthy Twin Study. Twin Res Hum Genet. 2014 Mar 11:1-6.
- Vyas S, Conduah A, Vyas N, Otsuka NY. The role of the first metatarsocuneiform joint in juvenile hallux valgus. J Pediatr Orthop B. 2010; 19(5):399-402.




{kind=link}