Ever wondered if you’re more likely to suffer foot blisters because of your age, weight, gender, ethnicity, or something else? I’ve searched the literature and dug up the answers. Some risk factors for foot blisters we’re certain about. For other, the research is either conflicting or inconclusive. I’ve summarised the findings in the table, but please read the summaries on each factor for more details.
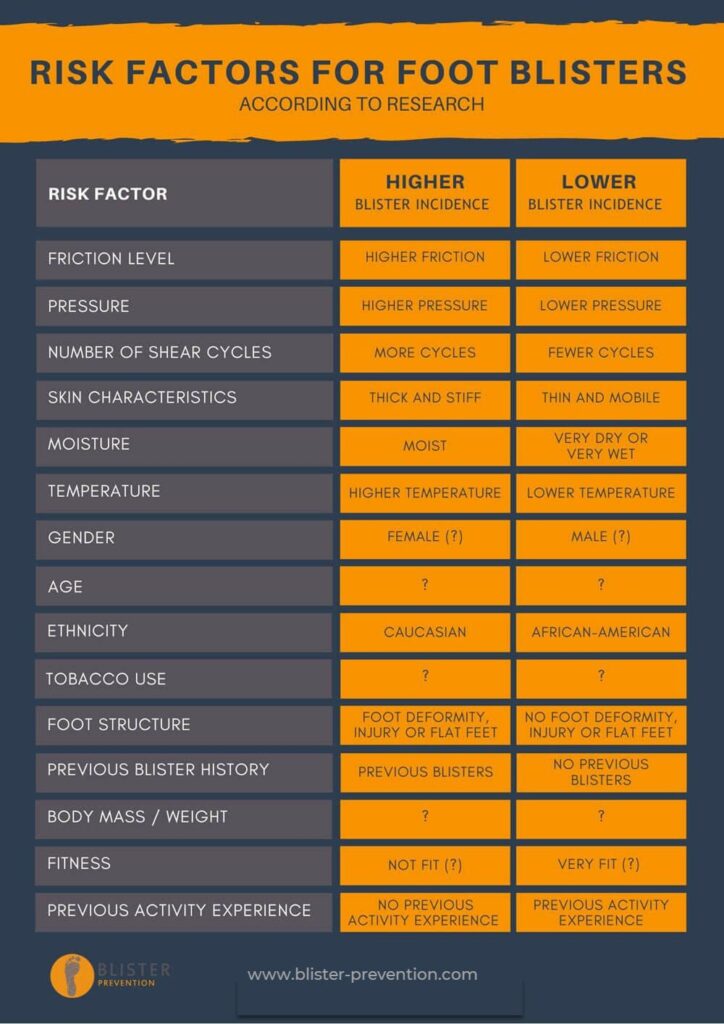
Here’s what we know about the risk factors for foot blisters
Friction, pressure and number of shear cycles
The combination of these factors are the most obvious risk factors for foot blisters. The magnitude of frictional forces and the number of times a material or object cycles over the skin determines the probability of blister development. The higher the COF the fewer the cycles necessary to produce a blister.³ ⁴ ⁵ ⁶ ⁷ In addition, heavy carried loads (higher pressure) have been shown to increase blister incidence.⁸ ⁹
Skin characteristics
Every experimental blister study has shown that blisters form most easily on thick and stiff skin of the feet, especially the soles¹⁰ ¹¹ as opposed to thinner skin on the rest of the body. It makes the skin on the soles, or acral skin, one of the most certain risk factors for foot blisters. This thicker skin is required to maintain the blister roof rather than have it shed off early in the process.
Skin moisture
It is well demonstrated that skin friction level increases in the presence of moisture, compared to very dry or very wet skin.³ ⁴ ¹⁰ ¹¹ ¹² ¹³ ¹⁴
Temperature
In almost every discussion you’ll read on blisters, heat is always mentioned as a causative factor, and rightly so. But heat is not required for blister development. The temperature-blister association is multifactorial.³ ⁵ ⁷ ¹⁰ ¹⁵ ¹⁶ Here’s why.
Ambient temperature?
Higher ambient temperatures cause more perspiration.⁴ And as you’d expect, increased walking speed causes higher in-shoe temperatures¹⁷ ¹⁸ which results in increased sweating.¹⁹ This perspiration provides a ‘moist’ environment, and a moist environment (neither very wet nor very dry) is known to increase friction coefficients³ ¹⁰ ¹³ which increases blister incidence⁶ ¹¹ by way of shear.⁵ Although blisters occur more readily in hot temperatures, blisters still occur in cold climates.¹⁵ ²⁰ Griffin¹⁵ produced experimental blisters on chilled, warmed and “normal” temperature skin and noted:
- blisters formed quicker when initial skin temperature was higher
- blisters took longer to form on chilled skin (14 degrees Celsius) compared to normal (30 degrees Celsius) and warmed skin (46 degrees Celsius)
- when the initial skin temperature was low, the skin temperature at the time of blistering was also lower
Second degree burn?
Some believe friction blisters to be a burn. However, research shows this not to be the case. Thermal burns that produce blisters are in fact second degree burns, and second degree burn blisters exist in a deeper layer of skin – the dermis. Additionally, friction blisters do not resemble thermal burns either clinically or histologically.⁴ ⁷ ¹⁵ ²¹ Research has found that rubbing causes only moderate increases in skin temperatures, to between 41 degrees and 50 degrees Celsius which are insufficient to cause a burn.³ ⁵ ⁷ ¹⁰ ¹⁵ ¹⁶ ²² ²³ ²⁴
Heat from rubbing?
The act of rubbing any two surfaces together causes the production of heat and it’s no different for the skin.¹⁶ ²⁵ Li¹⁶ demonstrated that rubbing causes a moderate increase in skin temperature, and that this warmer area of skin increases sweat production, which increases skin friction. However, this perspiration/friction mechanism [rubbing – heat – more sweat – higher friction – blister] is in contrast to the burn mechanism [rubbing – heat – burn – blister] and this distinction should be recognised.⁴ ⁵ ⁷ ¹⁰ ¹⁵ ¹⁶ ²³
Inflammation?
Hashmi et al²³ measured temperature changes during and after blister formation. They specifically aimed to minimise heat from rubbing, instead focusing on temperatures after blister formation. They demonstrated temperature increases due to inflammation, indicating heat is a result of the injury.⁷ ²³
Gender
There is conflicting research evidence regarding gender as one of the risk factors for foot blisters.
Some studies found women to be more susceptible: Patterson et al²² found women were 1.6 times more likely to blister. Brennan et al²⁶ found women were more likely: 47% vs 30%. And finally, Veijgen et al²⁷ found that women were more likely to have a higher skin coefficient of friction compared to men.
On the other hand, some studies have found no correlation between blisters and gender. Twombly and Schussman²⁸ showed an equal blister incidence of 46% for males and females. Boulware²⁹ showed similar blistering results for men (65%) and women (63%). Choi et al³⁰ found blister incidence to be equal between male and female. And Knapik et al³¹ found no differences. Skin friction studies by Cua et al,³² ³³ Savescu et al³⁴, Van Tiggelen et al³⁵ and Sivamani et al³⁶ found no skin friction differences between men and women.
Age
There is conflicting evidence on blister incidence and age. As a risk factor for foot blisters, Reynolds et al⁸ found a younger age to be a risk factor for blisters on a 5-day 161km cross country march of 218 light infantry males. Brennan et al²⁶ found 26-34 year olds were more likely to get blisters than younger and older troops. Yavuz and Davis³⁷ found that plantar shear is not dependent on age, comparing adult and pediatric subjects. Veijgen et al³⁸ found COF values highest in the over 50 years of age group compared to younger subjects. And Cua et al³² ³³ and Sivamani et al³⁶ found no COF differences in skin friction between young and old subjects.
Ethnicity
Patterson et al²², Reynolds et al⁸ and Van Tiggelen et al³⁵ found Caucasian ethnicity to be one of the risks factor for foot blisters compared to African-American. Knapik et al³¹ found “Individuals of black ethnicity were at significantly lower risk than those of white, Asian, Hispanic or ‘other’ ethnicities. There were no differences between white, Asian, Hispanic or ‘other’ ethnic groups”. But as far as skin friction research goes, Sivamani et al³⁶ found no skin COF measurement differences between Caucasian, African-American, Hispanic or Asian ethnicities.
Tobacco use
Reynolds et al⁸ found blisters were more likely to develop among tobacco cigarette smokers (but not in smokeless tobacco users). Knapik et al³¹ found the opposite. Van Tiggelen et al³⁵ did not find any association. The dury is out on whether tobacco is one of the significant factors for foot blisters
Foot structure
Van Tiggelen et al³⁵ found an increased blister incidence in those with orthopedic foot deformities. Other than “high arched or flat feet”, no information about these deformities is given. Knapik et al³¹ found a higher blister incidence in those that reported they had flat feet as opposed to normal feet. Earlier, Patterson et al²² demonstrated a 1.2 times elevated blister incidence if recruits had a history of low back / leg / foot injury.
Previous blister history
Previous history of blisters has been found to be a reliable indicator of blister risk by both Patterson et al²² and Brennan et al²⁶. Patterson et al²² found those who had experienced a foot blister in the previous 2 years were 3.6 times more likely to develop blisters during military training. Van Tiggelen et al³⁵ found there was a non-statistically significant increase in blister incidence when blisters were suffered the previous year. In my experience, previous blister experience is one of the most obvious risk factors for foot blisters, at that particular anatomical location.
Body mass / weight
Reynolds et al⁸ found a low body mass to be a risk factor for blisters. Jagoda et al³⁹ found body weight to be irrelevant. And finally, Patterson et al²² found height, weight and BMI did not influence blister development.
Fitness
There is conflicting evidence. Knapik et al³¹ found low aerobic fitness as a risk factor. Patterson et al²² found slower runners (over 16 minutes to run 2 miles) were 1.5 times more likely to suffer blisters during 6 weeks of military training, but overall physical fitness scores showed no association. Reynolds et al⁸ found physical fitness was not a risk factor for blisters.
Previous activity experience
Jagoda et al³⁹ found the amount of running a person does to be the most protective factor to foot blisters. Van Tiggelen et al³⁵ demonstrated that the lack of previous hiking experience was a risk factor for blisters in military personnel, suggesting this was a result of not having their “boots already broken in”, a lack of skin adaption and not knowing “how to manage their personnel equipment”, as did Knapik et al.³¹ Yet in the same study, Van Tiggelen³⁵ found no association between blister incidence during 6 weeks of basic military training and fitness based on hours of “sports practice” undertaken per week.
Caselli and Longobardi⁴⁰ found shear injury incidence (blisters, calluses and corns combined) was higher in marathon runners with lower training miles ran per week. Yavus and Davis³⁷ found that runners’ skin underwent more shear than non-runners. Edholm⁴¹ found a lack of heat acclimatization to also increase blister incidence. And Knapik et al³¹ found that a sickness in the last 12 months was a significant risk factor for blisters.
Definition of a risk factor
Remember, a risk factor does not necessarily imply causation. “Risk factors or determinants are correlational and not necessarily causal, because correlation does not prove causation.”¹ For example, we know that there is a statistical correlation between eating ice cream and drowning incidents, but ice cream consumption does not cause drowning. Where A and B are correlated, there are four possibilities:
- A is a cause of B
- B is a cause of A
- the correlation is pure coincidence
- A and B are connected by a common cause (like the ice-cream example, the common cause being hot weather)²
References
- “Risk factor”. Wikipedia – The Free Encyclopaedia (online). Available at http://en.wikipedia.org/wiki/Risk_factor
- Mumford Sand Anjum RL. 2013. Correlation is not causation (online). Oxford University Press’s Blog. Available at http://blog.oup.com/2013/ll/correlation-is-not-causation/
- Naylor P. 1955(A). The skin surface and friction. British Journal of Dermatology. 67: 259-48.
- Naylor P. 1955(B). Experimental friction blisters. British Journal of Dermatology. 67: 327-42.
- Comaish JS. 1973. Epidermal Fatigue as a Cause of Friction Blisters. The Lancet. January: 81-83.
- Akers WA. 1985. Measurement of Friction Injuries in Man. American Journal of Industrial Medicine. 8: 473-481.
- KnapikJJ, Reynolds K, Duplantis KL and Jones BH. 1995. Friction blisters – pathophysiology, prevention and treatment. Sports Medicine. Vol. 20(3) 136-147.
- Reynolds KL, White JS, Knapik JJ, Witt CE and Amoroso PJ. 1999. Injuries and risk factors in a 100 mile (161 km) infantry road march. Preventative Medicine. 28:167-173.
- Knapik J. 2000. Physiological, biomechanical and medical aspects of soldier load carriage. Research and Technology Organisation Human Factors and Medicine Panel Specialists’ Meeting. 27-29 June: KN1-19.
- Akers WA and Sulzberger MB. 1972.The Friction Blister. Military Medicine. 137:1-7.
- Sulzberger MB, Cortese TA, Fishman L and Wiley HS. 1966. Studies on blisters produced by friction. The Journal of Investigative Dermatology. 47(5) 456-465.
- Highley DR, Coomey M, DenBeste M and Wolfram LJ. 1977. Frictional properties of skin. The Journal of Investigative Dermatology. Vol 69 No 3: 303- 305.
- Nacht S, Close J, Yeung D and Gans EH. 1981. Skin friction coefficient: changes induced by skin hydration and emollient application and correlation with perceived skin feel. Journal of the Society of Cosmetic Chemists. 32 (March-April): 55-65.
- Sivamani RK, Goodman J, Gitis NV, Maibach HI. 2003(A). Coefficient of friction: Tribological studies in man – an overview. Skin Research and Technology. 9(3): 227-34.
- Griffin CPT, Cortese TA, Layton LL and Sulzberger MB. 1969. Inverse time and temperature relationship in experimental friction blisters. The Journal of Investigative Dermatology. 52 (Morning Session): 384-401.
- Li W, Pang Q, Jiang Y, Zhai Z and Zhou Z. 2012. Study of physiological parameters and comfort sensations during friction contacts of the human skin. Tribological Letters. 8:1-12.
- Covill D, Guan Z, Bailey M and Pope D. 2003. Effects of varying the environmental conditions on in-shoe temperature (online). Available at http://www.staffs.ac.uk/isb-fw/Abstracts/COVILL_EFFECTS_OF.pdf
- Hall M, Shurr DG, Zimmerman MB and Saltzman CL. 2004.Plantar foot surface temperatures with use of insoles. The Iowa Orthopaedic Journal. 24:72-75.
- Deng F, Gong T, Jin H and Du S. 2009. Research on factors influencing temperature and relative humidity inside of shoes (online). College of Resources and Environments. Available at http://www.aaqtic.org.ar/congresos/china2009/download/2-6/2-218.pdf
- Knapik J, Reynolds K, Staab J, Vogel JA and Jones B. 1992. Injuries associated with strenuous road marching. Military Medicine. 157: 64-67
- Cortese TA, Griffin TB, Layton LL and Hutsell TC. 1969. Experimental friction blisters in macaque monkeys. The Journal of Investigative Dermatology. Vol 53 No 2:172-177.
- Patterson HS, Woolley TW and Ledner WM. 1994. Foot blister risk factors in an ROTC summer camp population. Military Medicine. 159(2): 130-5.
- Hashmi F, Richards BS, Forghany S, Hatton Aland Nester C. 2013. Skin Research and Technology. 19: e479-e489.
- KnapikJJ. (undated). Friction blisters: pathophysiology, risk factors and prevention. US Army Center for Health Promotion and Preventative Medicine. 1-4.
- El-Shimi AF. 1977. In vivo skin friction measurements. Journal of the Society of Cosmetic Chemists. 28 (Feb): 37-51.
- Brennan FH, Jackson CR, Olsen C and Wilson C. 2012. Blisters on the battlefield: the prevalence of and factors associated with foot friction blisters during operation Iraqi freedom. Military Medicine. 177 (2): 157-162.
- Veijgen NK, Masen MA and Van der Heide E. 2013(A). Relating friction on the human skin to the hydration and temperature of the skin. Tribological Letters. 49:251-262.
- Twombly SE and Schussman LC. 1995. Gender differences in injury and illness rates on wilderness backpacking trips. Wilderness and Environmental Medicine. 4: 363-76.
- Boulware DR. 2004. Gender differences among long-distance backpackers: a prospective study of women Appalachian trail backpackers. Wilderness and Environmental Medicine. 15:175-180.
- Choi S-C, Min Y-G, Lee l-S, Youn G-H, Kang B-R, Jung Y-S, Cho J-P and Kim G-W. 2013. Injuries associated with the 580km university student grand voluntary road march: focus on foot injuries. Rehabilitation and Sports Medicine. Journal of Korean Medical Science. 28:1814-1821.
- Knapik JJ, Reynolds K and Barson J. 1999. Risk factors for foot blisters during road marching: tobacco use, ethnicity, foot type, previous illness and other factors. Military Medicine. 164: 92-97.
- Cua AB, Wilhelm KP and Maibach HI. 1990. Frictional properties of human skin: relation to age, sex and anatomical region, stratum corneum hydration and transepidermal water loss. British Journal of Dermatology. Volume 123, Issue 4: 473-479.
- Cua AB, Wilhelm KP and Maibach HI. 1995. Skin surface lipid and skin friction: relation to age, sex and anatomical region. Skin Pharmacology. Vol8 No 5: 246-251.
- Savescu AV, Latash ML and Zatiorsky VM. 2008. Atechnique to determine friction atthe fingertips. Journal of Applied Biomechanics. 24: 43-50.
- Van Tiggelen D, Wickes S, Coorevits P, Dumalin M and Witvrouw E. 2009. Sock systems to prevent foot blisters and the impact on overuse injuries of the knee joint. Military Medicine. 174 (2): 183-9.
- Sivamani RK, Wu GC, Gitis NV, Maibach HI. 2003(C).Tribological testing of skin products: gender, age and ethnicity on the volar forearm. Skin Research and Technology. 9(4): 299-305.
- Yavuz M and Davis BL. 2010. Plantar shear stress distribution in athletic individuals with frictional foot blisters. Journal of the American Podiatric Medicine Association. 100(2): 116-120.
- Veijgen NK, Van der Heide E and Masen MA. 2013(C). A multivariable model for predicting the frictional behaviour and hydration of the human skin Skin Research and Technology. Vol 19 Issue 3 (August): 330-338.
- Jagoda A, Madden H and Hinson CA. 1981. Friction blister prevention study in a population of marines. Military Medicine. 146(1): 42-44
- Caselli MA and Longobardi SJ. 1997. Lower extremity injuries at the New York City marathon. Journal of the American Podiatric Medical Association. Vol 87 No 1: 34-37
- Edholm OG. 1969. The effect of heat on acclimatized and unacclimatized groups of fit men. Journal of the Royal Society of Medicine. Vol 62:1175-1179.